
Sciatica pain affects up to 40% of adults at some point. Most never identify the specific cause behind their nerve pain.
Table of Contents
ToggleSpine and Posture Care in Sydney sees hundreds of patients each year with radiating leg pain and no clear diagnosis. The problem is rarely the sciatic nerve itself. Something deeper in the lower back, pelvis, or hip is almost always driving the compression.
Understanding what that something is makes the difference between chasing sciatica symptoms and actually fixing the problem.
How Sciatica Develops in the Lower Back
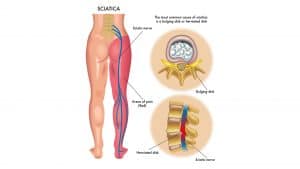
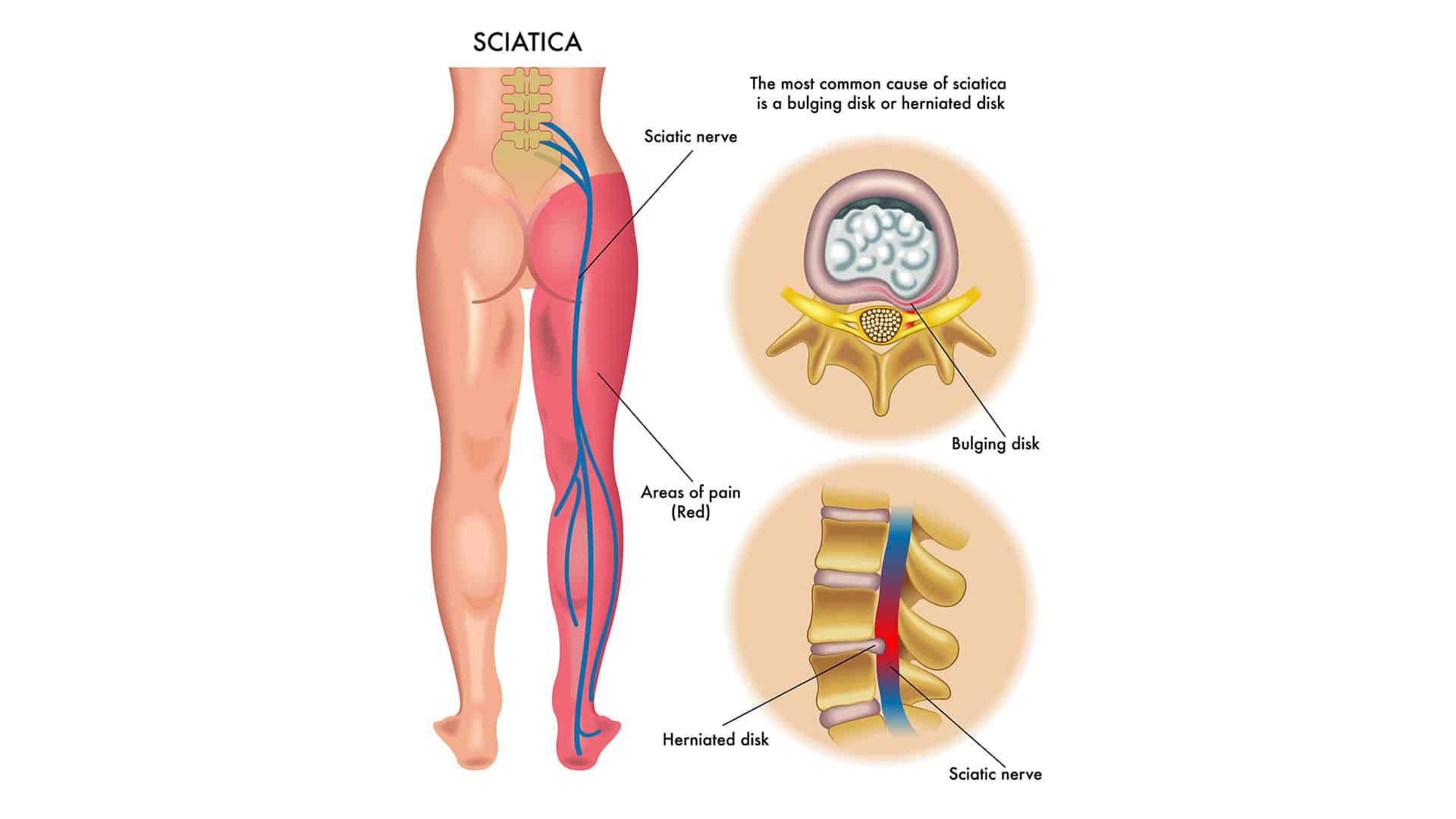
The sciatic nerve is the longest and thickest nerve in the body. It forms from five nerve roots in the lumbar and sacral spine: L4, L5, S1, S2, and S3. These roots merge into a single nerve trunk behind the pelvis. The nerve then runs down the back of each leg to the knee. Below the knee it branches into the tibial and peroneal nerves. These branches control sensation and movement in the lower leg and foot.
Sciatica is not a condition on its own. It is a symptom of a structural or muscular problem that compresses one or more nerve roots. The location and severity of the compression determine where the pain travels.
Most sciatica causes start in the lower lumbar spine at L4-L5 or L5-S1. These two levels bear the most body weight. They also handle the most rotational stress. That combination makes them vulnerable to disc injuries, joint wear, and nerve compression. Getting an accurate diagnosis through sciatica treatment in Sydney matters because each cause needs a different approach.
Herniated or Bulging Disc
A herniated disc is the most common cause of sciatica. Research in the New England Journal of Medicine confirms disc herniation accounts for roughly 90% of cases in adults under 50.
Spinal discs sit between each vertebra and absorb shock. Each disc has a tough outer ring (annulus fibrosus) and a soft centre (nucleus pulposus). When the outer ring tears, the inner material pushes outward. It then presses against a spinal nerve root.
How a Disc Herniation Causes Nerve Compression
The herniated material does not need to be large to cause pain. Even a small protrusion at L4-L5 or L5-S1 can compress the nerve root. The result is shooting pain, tingling, or numbness down the leg. Chemical irritation from the disc material also triggers inflammation. That inflammation amplifies the pain signal further.
Heavy lifting with poor form, sudden twisting, and repetitive bending are common triggers. Prolonged desk or vehicle sitting also raises risk. Sustained spinal flexion increases pressure on the posterior disc wall. Recognising bulging disc symptoms in the lower back early can prevent a minor bulge from becoming a full herniation.
Spinal Canal Stenosis
Spinal stenosis is a narrowing of the spinal canal. The spinal canal is the bony tunnel that protects the spinal cord and nerve roots. As it narrows, the space for the nerves shrinks. Compression and inflammation follow.
This cause is far more common in adults over 50. Thickened ligaments, bone spurs, and disc dehydration reduce the canal width over time. Spine and Posture Care treats stenosis patients at the Macquarie Street and Barangaroo clinics in Sydney CBD. The condition often responds well to conservative care when caught early.
Central vs Lateral Stenosis
Central stenosis narrows the main spinal canal. It can compress multiple nerve roots at once. Lateral stenosis narrows the foramen, the side openings where nerves exit the spine. It typically affects one nerve root on one side. Lateral stenosis at L5-S1 is a frequent cause of single-leg sciatica in older adults.
Stenosis-related sciatica often worsens with standing and walking. It improves with sitting or bending forward. This pattern is called neurogenic claudication. It separates stenosis from disc-related sciatica, where sitting makes pain worse. Patients seeking lower back pain treatment often discover stenosis as the true driver of both back and leg pain.
Piriformis Syndrome
Piriformis syndrome is an underdiagnosed cause of sciatica. It starts in the buttock rather than the spine.
The piriformis is a small, flat muscle. It runs from the sacrum (the bone at the base of the spine) to the greater trochanter on the outer hip. The sciatic nerve passes directly beneath this muscle in most people. In about 15 to 17% of the population, the nerve pierces through the muscle belly. Those individuals are especially vulnerable to compression.
What Causes the Piriformis to Tighten
A piriformis spasm, swelling, or chronic tightness presses against the sciatic nerve. The result is pain that radiates down the back of the leg. The pattern mimics spinal sciatica closely. That similarity is why piriformis syndrome is frequently misdiagnosed.
Prolonged sitting on hard surfaces is a common trigger. Repetitive hip rotation from running or cycling also contributes. Direct trauma to the buttock and biomechanical imbalances like flat feet or leg length differences are additional causes. A chiropractor can differentiate piriformis syndrome from lumbar disc sciatica using the FAIR test and Pace test.
Spondylolisthesis
Spondylolisthesis occurs when one vertebra slips forward over the one below it. The slippage narrows the space for nerve roots. It can compress the sciatic nerve at its exit point.
The most common level is L5 slipping forward on S1. Two groups are most affected. Younger athletes in sports with repeated hyperextension (gymnastics, cricket, fast bowling, football) develop it from stress fractures. Older adults develop it through joint degeneration over time.
Grading the Slip
The slip is graded from Grade I (up to 25% slippage) to Grade IV (76 to 100%). Grade I and II slips are the most common. They often respond to spinal adjustments, core strengthening, and postural correction. Grade III and IV slips may need surgical consultation. Spine and Posture Care uses diagnostic imaging to grade the slip before recommending a treatment plan.
Degenerative Disc Disease
Degenerative disc disease is not a disease in the traditional sense. It describes the natural wear-and-tear that affects spinal discs over time.
Discs lose hydration and height with age. The vertebrae move closer together as a result. This reduced spacing compresses the nerve exit points (foramina). It can irritate the sciatic nerve roots. Degenerated discs may also develop small tears. These tears leak inflammatory proteins onto nearby nerves. The result is chemical radiculitis without any visible structural compression on imaging.
Risk Factors for Accelerated Degeneration
Smoking is one of the strongest modifiable risk factors. Nicotine restricts blood flow to the discs. It accelerates breakdown of disc tissue. Obesity places extra mechanical load on the lumbar spine. It speeds up disc height loss. Repetitive heavy lifting, vibration exposure from truck driving or heavy machinery, and prolonged static postures also contribute.
The Better Health Channel notes that degenerative changes are the most common sciatica cause in adults over 60. The condition often coexists with stenosis and facet joint arthritis. That combination creates multiple nerve compression sources at once.

How Poor Posture and Lifestyle Habits Trigger Sciatica
Poor posture does not herniate a disc overnight. It creates the conditions that lead to disc and joint problems over months and years.
Slouched sitting increases intradiscal pressure in the lumbar spine by up to 40%. Sustained pressure weakens the posterior disc wall over time. It accelerates degeneration at the L4-L5 and L5-S1 levels. Forward head posture and rounded shoulders shift the centre of gravity forward. The lumbar spine then compensates with excessive lordosis or flexion. Both patterns overload the lower lumbar segments.
Occupational and Lifestyle Risk Factors
Desk workers who sit 8 or more hours daily without movement breaks face higher sciatica risk. Drivers and truck operators add whole-body vibration to that equation. Multiple studies link vibration exposure to accelerated lumbar disc degeneration.
Physical inactivity is another factor. Weak core muscles fail to stabilise the spine. Excess body weight adds pressure, with each extra kilogram placing roughly 4 kilograms of load on the lumbar discs. A poor mattress that does not support the natural spinal curve also contributes. Identifying bad posture warning signs early reduces the cumulative damage that leads to nerve compression.
Sciatica Causes in Women: Pelvic and Pregnancy-Related Triggers
Women experience sciatica at similar rates to men. However, several causes are unique to or more common in women.
During pregnancy, the growing uterus shifts the centre of gravity forward. Lumbar lordosis increases as a result. The hormone relaxin loosens pelvic ligaments for delivery. It also reduces spinal joint stability. These changes compress lumbar nerve roots. Sciatica is most common in the second and third trimesters. It can persist after delivery if core stability and pelvic alignment are not restored.
Pelvic Causes of Sciatica in Women
Endometriosis, ovarian cysts, and pelvic inflammatory conditions can refer to pain along the sciatic nerve path. The pattern mimics true spinal sciatica. Piriformis syndrome is also more prevalent in women. Wider pelvic anatomy changes the angle where the piriformis crosses the sciatic nerve. A thorough assessment of both spinal and pelvic sources is essential for women with these symptoms.
Sciatica Causes Comparison Table
| Cause | Primary Location | Age Group Most Affected | Key Symptom Pattern | Typical Recovery |
|---|---|---|---|---|
| Herniated/Bulging Disc | L4-L5, L5-S1 disc | 25 to 50 | Worse sitting, bending | 6 to 12 weeks |
| Spinal Stenosis | Central or lateral canal | 50+ | Worse standing, walking | Ongoing management |
| Piriformis Syndrome | Buttock/piriformis muscle | 30 to 50 | Deep buttock pain, worse sitting | 4 to 8 weeks |
| Spondylolisthesis | L5-S1 vertebral slip | Young athletes, 50+ | Worse with extension | 8 to 16 weeks |
| Degenerative Disc Disease | Multi-level lumbar | 60+ | Gradual onset, stiffness | Ongoing management |
| Posture/Lifestyle | L4-L5, L5-S1 | 25 to 55 (desk workers) | Worse after prolonged sitting | 4 to 8 weeks |
| Pregnancy/Pelvic | Lumbar and pelvis | Pregnancy, 25 to 40 | Second/third trimester onset | Resolves post-delivery |
Conclusion
Sciatica has multiple causes, and each one responds to a different treatment approach. A plan built for piriformis syndrome will not help stenosis. Exercises that relieve a disc bulge may worsen spondylolisthesis. That is why identifying the specific source of nerve compression matters more than treating the pain alone. Most cases resolve within 4 to 12 weeks once the right cause is addressed. Sciatica with progressive leg weakness, groin numbness, or bladder changes needs immediate medical attention.
Spine and Posture Care helps patients in Sydney CBD connect the diagnosis to a targeted recovery plan. Combining clinical treatment with the right sciatica exercises and stretches speeds recovery and lowers the chance of recurrence.
Frequently Asked Questions
Can bad posture cause sciatica?
Bad posture does not cause sciatica instantly. It creates the spinal conditions that lead to nerve compression over time. Slouched or forward-leaning sitting increases lumbar disc pressure by up to 40% compared to standing. Over months and years, this weakens the disc wall at L4-L5 and L5-S1. These are the two segments most commonly involved in sciatica. Desk workers in Sydney CBD who sit 8 or more hours daily face particularly high risk. Correcting posture, strengthening the core, and taking regular standing breaks reduce the strain that leads to disc herniation and nerve irritation.
How does sciatica start?
Sciatica starts when something compresses a nerve root in the lower back. The five nerve roots (L4, L5, S1, S2, S3) form the sciatic nerve. A herniated disc is the most common trigger. The soft inner material pushes through a tear in the outer wall and presses against the nerve. Other causes include spinal canal narrowing (stenosis), a tight piriformis muscle, or a slipped vertebra (spondylolisthesis). The compression sends pain, tingling, or numbness from the lower back down the leg. Most cases begin after heavy lifting, sudden twisting, or prolonged poor sitting posture.
Is pelvic pain related to sciatica?
Pelvic pain and sciatica are closely connected. The sciatic nerve passes through the pelvic region between the lumbar spine and the leg. Pelvic conditions can compress or irritate the nerve directly. Piriformis syndrome, where the buttock muscle spasms against the sciatic nerve, is one common pelvic cause. In women, pregnancy pelvic changes, endometriosis, and ovarian cysts can produce pain along the sciatic nerve path. A clinical assessment should examine both the lumbar spine and pelvis to find the true source.
What is the main cause of sciatica in women?
The main cause is the same as in men: a herniated or bulging lumbar disc, usually at L4-L5 or L5-S1. Women face several additional risk factors. Pregnancy shifts the centre of gravity and loosens pelvic ligaments through the hormone relaxin. Both changes compress lumbar nerve roots. Wider pelvic anatomy in women alters the piriformis angle across the sciatic nerve. This makes piriformis syndrome slightly more common. Endometriosis and large ovarian cysts can also refer pain along the sciatic path. Women with sciatica during or after pregnancy should have both spine and pelvis assessed.
Can sciatica go away on its own?
Mild sciatica can resolve within 4 to 6 weeks without treatment. This is most likely when the cause is a minor disc bulge or temporary muscle spasm. The body can reabsorb small disc herniations over time. Sciatica lasting beyond 4 weeks, or with progressive numbness, weakness, or sleep disruption, is unlikely to resolve alone. Conservative care through chiropractic treatment, exercise, and postural correction resolves 80 to 90% of cases without surgery. Leaving moderate sciatica untreated risks chronic nerve damage and muscle wasting. Early diagnosis produces faster recovery.
Why does sciatica cause pulsating pain?
Pulsating sciatica pain signals active inflammation around the nerve root. When a herniated disc presses on a nerve, the disc material releases inflammatory chemicals. These include cytokines and phospholipase A2. The chemicals irritate the nerve sheath and make it hypersensitive. That produces a pulsating or throbbing sensation, often in sync with blood flow. The pulsating quality is more common at night or after sitting. Reduced movement allows inflammatory fluid to pool around the nerve. Ice, anti-inflammatory strategies, and gentle movement help reduce the irritation. Persistent pulsating sciatica should be assessed to rule out significant nerve compression.